
A new report from the Center for Research on the Wisconsin Economy has stirred debate about whether Wisconsin, which has taken great pride in being at the forefront of health care price transparency, is actually serving health care consumers well.
The CROWE report, “Rising Health Care Costs in Wisconsin: The Case for Price Transparency,” claims employers are paying far more than necessary for medical insurance because the system does not function like a competitive market.
Its authors say better tools — especially price transparency and smarter benefit design — could generate savings without reducing quality.
Executives representing Wisconsin hospitals and insurers questioned the accuracy of the report, took issue with its recommendations and touted consumer price and quality tools they say put Wisconsin on the cutting edge of health care consumerism.
Center of attention
The report was co-authored by Ananth Seshadri, the chair and co-director of the center, which was established in 2017 within the Department of Economics at the University of Wisconsin-Madison. Its mission is to disseminate economic policy research from a market perspective, with an emphasis on the Wisconsin economy.

The report focuses on hospital costs because hospitals, which drove 31% of the nation’s estimated $4.9 trillion in overall health care costs in 2023, are the largest single component of health care spending — more than pharmaceutical costs, physician services and other services.
According to the report, 69% of Wisconsin employers say rising health care costs have forced them to cut hiring and investment, reduce compensation or raise prices.
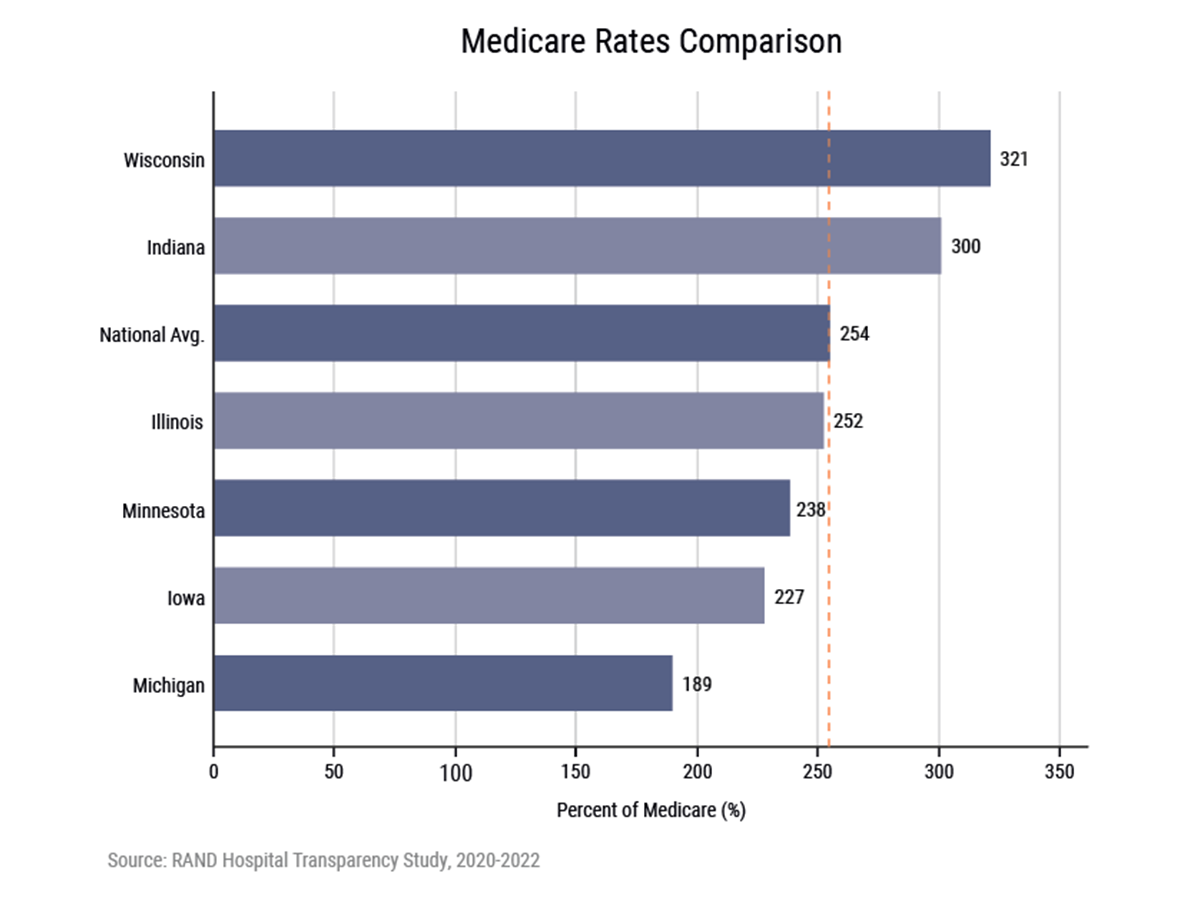
In Wisconsin, it says family health insurance premiums have exploded 365% since 1999, from $5,809 to $26,993, and Wisconsin hospitals now charge the fourth-highest prices in the nation at 321% of Medicare rates, which is the highest among Midwest states.
The report cites a 2024 RAND Corp. hospital price transparency study which compares commercially negotiated hospital prices to Medicare payment rates across the country. It found that Wisconsin hospitals charge an average of 321% of Medicare rates. This places the state fourth highest nationally and highest in the Midwest, well above the national average of 254%.
Private insurers therefore pay more than three times what Medicare pays for the same services, and those costs are passed on to Wisconsin employers and employees, the study says.
Seshadri said in an email that employers still pay about 75% of premiums on average, making them the primary bearers of cost increases. As a result, 69% of Wisconsin employers report real economic consequences, including reduced hiring, lower capital investment, slower wage growth and higher product prices.
“Health care costs are a major and growing constraint on business performance,” Seshadri said. “Health insurance is now one of the largest components of total compensation, and its rapid growth is directly affecting firm behavior.”
Seshadri said the bottom line is that health care costs are not just a benefits issue — they act like a tax on labor and business activity, directly reducing competitiveness, especially relative to lower-cost states.
To fix the problem, the report recommends improving price transparency by mandating full federal compliance, building a state-sponsored price-comparison tool, creating a mandatory all-payer claims database, and strengthening antitrust scrutiny of hospital mergers, which the report contends is contributing to cost increases by reducing competition.
The report also points to significant cost variation for the same procedure across Wisconsin hospitals, yet patients and employers rarely see these prices despite a federal mandate to publicly report hospital charges.
For example, the report said median negotiated rates for a diagnostic colonoscopy range from around $1,469 at Marshfield Clinic/Sanford Health to more than $4,600 at Froedtert Hospital in Milwaukee.
Seshadri said the cost of the same procedure can differ by 2 to 3 times across hospitals within Wisconsin, and these differences are not well explained by quality, but by market power and weak competition.
“Employers are overpaying due to price opacity and lack of effective purchasing leverage,” Seshadri said. “A key driver of high costs is not just overall inflation, but extreme and largely hidden price variation across providers.”
Seshadri also said employers (via insurers) often do not steer patients to lower-cost providers, they rarely see meaningful price signals, and existing benefit designs (copays and coinsurance) often fail to reflect price differences.
Since consumers are often unaware of these price differences, Seshadri said they cannot direct their health care spending toward lower-cost, higher-value providers.
The report recommends making actual negotiated prices accessible to consumers.
Medicare share
Since Medicare rates are set administratively by the Centers for Medicare & Medicaid Services and are uniform across payers within a geographic area (adjusted for local input costs), the authors say they provide a consistent benchmark for cross-state comparison.

Kyle O’Brien, president and CEO of the Wisconsin Hospital Association, said Medicare pays below the cost of treating patients, forcing hospitals to charge commercial payers more. O’Brien said Medicare payments to hospitals underfund hospitals nationally by $3.7 billion per year, and Medicaid payments to hospitals underfund hospitals by about $1.3 billion per year.
Medicare is the federal government’s health insurance program for people age 65 and older. Medicaid is a joint federal and state program that helps low-income individuals and families pay for their medical costs.
O’Brien said using Medicare benchmark rates does not provide an accurate representation of what’s needed to deliver health care in Wisconsin.
“Wisconsin is disadvantaged compared to other states through Medicare reimbursement, through a variety of means, including the area wage index and a lot of other things that get baked into what Medicare reimbursement is in this state,” he said. “So, when you have rates that are so low, you can’t accurately compare states because states are reimbursed at different rates.”
Under the CMS Hospital Price Transparency Rule, which went into effect on Jan. 1, 2021, all U.S. hospitals must publish machine-readable files containing at least four types of standard charges. Of these four types of charges, payer-specific negotiated rates are considered the most meaningful because they reflect what insurers, employers and employees actually pay.
The rule also requires hospitals to display, in a consumer-friendly, plain language format, the prices for at least 300 common “shoppable” services that can be scheduled in advance.
While the rule is designed to increase market competition, empower consumers to compare costs, and ultimately drive down health care expenses, not everyone believes hospitals comply.
The CROWE report cites a 2024 Urban Milwaukee article that said only 30-40% of Wisconsin hospitals are in full compliance, but the WHA’s O’Brien took issue with that.
O’Brien said the hospital industry has established three consumer tools, including one that is more of a quality tool than a price tool. He said the WHA’s PricePoint tool was one of the first tools in the country where hospitals came together and publicly posted their charges online.
After PricePoint, O’Brien said WHA developed CheckPoint, a quality transparency tool that showcases various hospital quality metrics, enabling patients to compare prices and performance from a quality perspective.
He said WHA also created Price Finder, which allows people to navigate directly to hospital price transparency web pages and access hospital specific contracted rates and price estimator tools.
“This (CROWE) report, just like other kinds of claims about Wisconsin’s compliance with price transparency regulations, is simply false,” O’Brien said. “There is not one hospital in Wisconsin that has been fined for noncompliance by the Centers for Medicare, Medicaid Services for not complying with this federal price transparency regulation.”
O’Brien said the hospital association encourages people to view their prices online through the tools hospitals provide, consistent with federal regulations.
“We really encourage patients to pick up the phone and work with the financial counseling staff at your local hospital to understand how your coverage will work in that facility,” he said.
Claiming data
From the standpoint of comparing prices, the CROWE report also said health care consumers would benefit from a mandatory all-payer claims database, which it lacks. The authors say establishing one should be a legislative priority, but legislation (Senate Bill 833) to do that failed to pass in the most recent legislative session.

Rachel Ver Velde, associate vice president of government relations and senior political advisor for Wisconsin Manufacturers & Commerce, a statewide chamber of commerce, said WMC supported SB 833 because the state needs a consumer-facing price tool. That includes an all-payers claims database with an aggregated dashboard to help employers access it and understand it.
“Our members, employers throughout Wisconsin, have said that you need to have the ability to shop around for care,” Ver Velde said. “It makes more informed consumers but it also helps employers help their employees navigate the complex health system, whether that be looking for the differences in price or even the differences in quality.
“So, not only do we think that there needs to be full hospital price transparency at the state level, but we also feel that there needs to be transparency by an all payers claims database, a database that has an outward looking dashboard that’s public-facing so people can use and compare that care based on cost and quality,” Ver Velde said.

Dana Richardson, CEO of the Wisconsin Health Information Organization, said WHIO operates a voluntary claims database and only two insurers that do business in Wisconsin do not submit data, but one of those holdouts is the largest — Anthem Blue Cross Blue Shield.
Richardson supports a mandatory all payers claims database in Wisconsin but said it should not be limited to hospital claims.
“I understand the rationale because that’s the most expensive component of health care, but we’re leaving a lot on the table,” Richardson said.
Richardson said WHIO looks at health care costs in what she called “episodes of care,” which include all of the care that’s provided before a hospital procedure, during hospitalization and afterward.
“This also then includes the fees that are paid to all of the physicians that are involved and other testing and maybe rehab and medications,” she said. “The reason why that’s important is because it gives you a more complete picture of what something actually costs.”
Richardson said the other advantage of this approach is the detailed breakdown. “Where are we actually spending the most money? Are we spending a lot of money on physicians or on testing or is it the procedure itself?” she said. “It isn’t always the procedure that is the most important or most expensive component.
“So, we really encourage the use of these episodes (of care),” she said. “We have several organizations that receive that data from us so that they can look at costs from a more complete picture.”
WHIO’s focus is on helping employers, health plans and brokers — not individual consumers — make sense of price data. “Not because consumers aren’t important, but a lot of health care decisions, when it comes to price, are actually made by employers and health plans,” she said. “So, that is a group that has been asking for more price transparency from the WHIO, and so we’ve really been working in that direction.
“There’s a group of consumers who can make awesome decisions about their health care, but there’s a lot of people for whom health care is just really complicated,” she said. “There’s a lot of weird lingo and the pricing structures are very odd, so our focus has been more on providing the information to the buyers so that they can use it for contract negotiations, but also in the design of their benefit plans.”
Network issue
John Nygren, CEO of the Wisconsin Association of Health Plans, questioned the practicality of having individual consumers compare prices for medical procedures, given that insurers negotiate rates for employer groups and that individuals are discouraged from seeking services outside of their network.

While an individual consumer may shop for medical care, if they receive a service outside of their network, it might not be covered by their insurance, and it may not be applied to their annual deductible.
Covering only in-network procedures is considered a cost-control measure because it allows insurance companies to leverage negotiated, discounted rates with health care providers. By restricting coverage to contracted providers, insurers avoid higher, uncontrolled fees charged by out-of-network providers.
“Our members work with employers to find ways to control costs, whether that be narrow networks, whether that be cost sharing, etcetera,” Nygren said. “The funny thing about all that is the consumer in general, when it comes to the tools that insurers have that control costs (co-pays and deductibles), they don’t like them.
“We’re the only part of this whole health care world that is incentivized to control costs,” Nygren said. “The consumer, as long as they’ve got their copay or their deductible, they’re covered.
“With providers, there’s a financial incentive on their side,” he said. “We’re the only one that’s really looking at controlling costs as part of doing business.”
Input cost
WHA’s O’Brien defended hospitals from a business standpoint, saying hospital input costs associated with delivering care have increased dramatically. He said the industry has seen double-digit increases related to labor and supply costs, and pharmaceutical charges also have risen significantly.
“Meanwhile, hospital price growth across the country has only gone up 3.3% in 2025 compared to all these other significant cost increases that hospitals bear,” he said.
He said when prices for hospital input costs go up, it doesn’t mean hospitals can just recoup those costs because oftentimes they are in multiyear contracts with payers that have rates that are established for a longer period.
“The important thing to understand is that the primary drivers of hospital costs are the inputs that go into delivering hospital care, which frankly are increasing at a significant rate,” he said.
O’Brien said hospitals have to care for everybody regardless of their ability to pay.
“So, if we have somebody that walks through an emergency department, and they’re not covered or they’re on a government program that underfunds the hospital for services that are provided, they have to make that up in some other place,” he said.